Very interesting report from Cal Skinner.

With all the talk about consolidating government, I’ve been wondering why McHenry County still has a Tuberculosis District.
It is financed with $250,000 of property tax dollars a year.
TB Districts were the first public health districts in Illinois.
McHenry County did not create its own Health Department until the mid-1960’s. (My home county on the Eastern Shore of Maryland had a health department before I was born in 1942.)
In the 1980’s then County Board member Ann Hughes got a referendum on the ballot to abolish the TB District, but that failed.
I recently took a look at the meeting packet of the TB District and found an extraordinary story.
McHenry County’s Health Department dealt with a case of drug resistant tuberculosis of nationwide significance in May and June.
How important was it?
The New York Times wrote a big story about it entitled, “Indian Woman Being Treated in U.S. for Drug-Resistant Tuberculosis.

Susan Karras
Quoted was Susan Karras, the Health Department’s Communicable Disease Coordinator.
A woman recently from India via Missouri and Tennessee sought medical help from a local hospital.
When diagnosed with tuberculosis, the Health Department arranged for her medical care to be provided by a National Institutes of Health hospital near Washington.
Federal taxpayers foot the bill there, according to Anthony Fauci, head of the agency, “Everything is free at the N.I.H. No one pays,” the New York Times reported.
Karras told me that the County paid to fly her to the National Institute of Health facility in Bethesda, Maryland.
The air ambulance cost $12,000.
McHenry County Health Department Director Michael Hill explained what happened:

Mike Hill
Because we were able to get this patient to NIH (this involved going all the way to the President’s office [by the CDC]) the direct costs to us were minimized.
I was able to get the air transport done for $12,000 (quotes ranged up to $35,000 from the few companies who were willing to do it).
I can’t complain about the federal government in this case since the patient’s treatment by NIH probably will end up in the hundreds of thousands of dollars, and the feds took on that expense.
If the county had to absorb the cost of this patient’s treatment, it would have been financially crippling for the TB program.
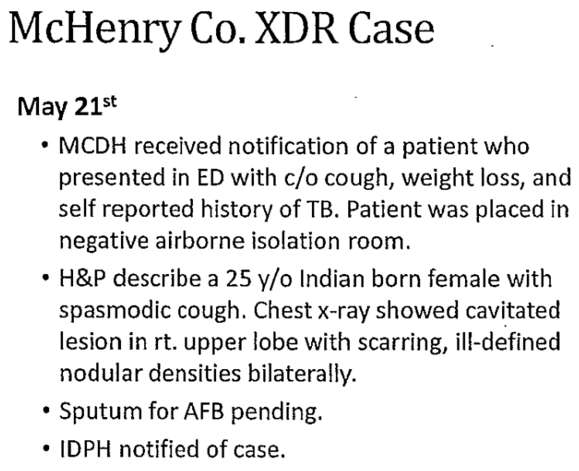
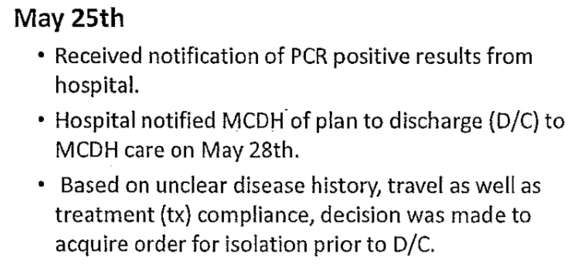
Below is the summary of the case that caught my attention.


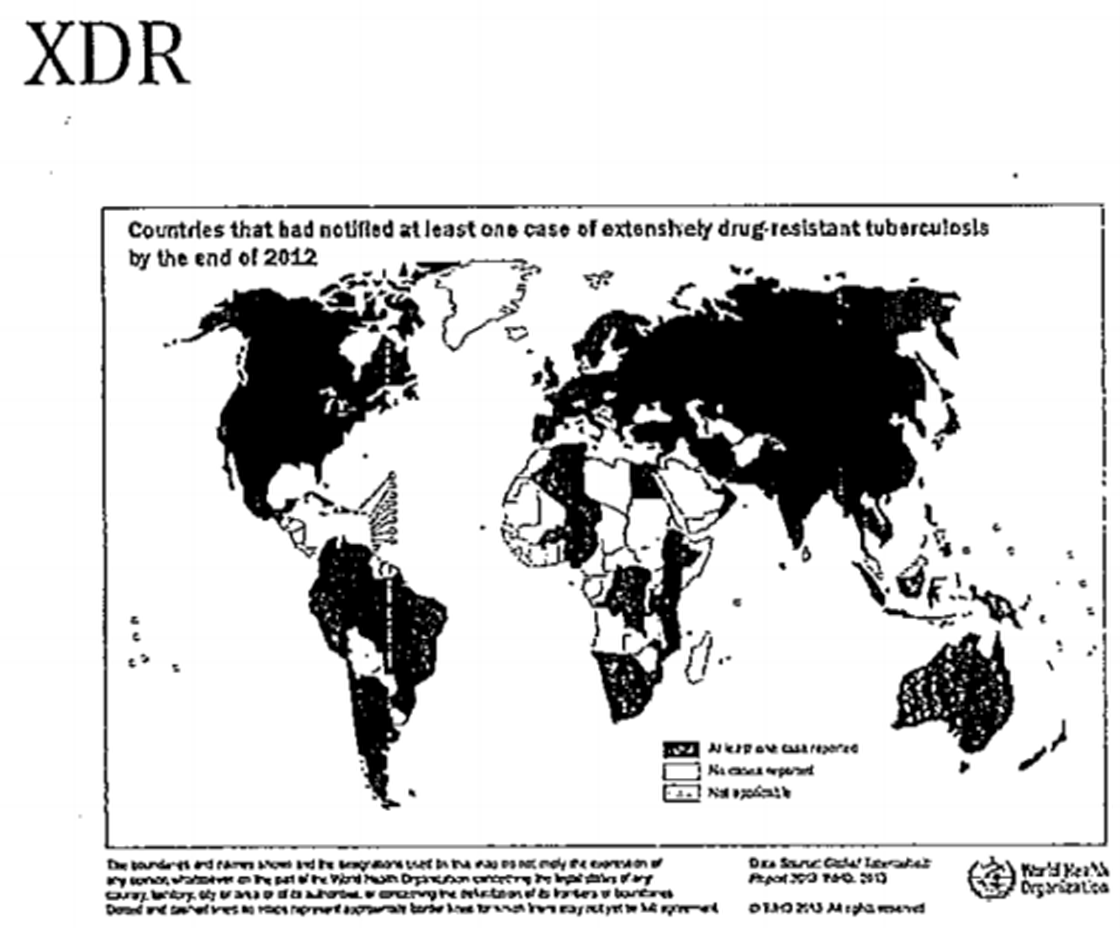
Spread of the type of tuberculosis treated in McHenry this summer.




Additional Daily Reports are available at: http://mchenrycountyblog.com/2015/11/25/mchenry-county-center-of-dangerous-tb-case/
On June 5th, the Health Department sent out the following press release on the matter:
Health Department reports case of extensively drug-resistant tuberculosis
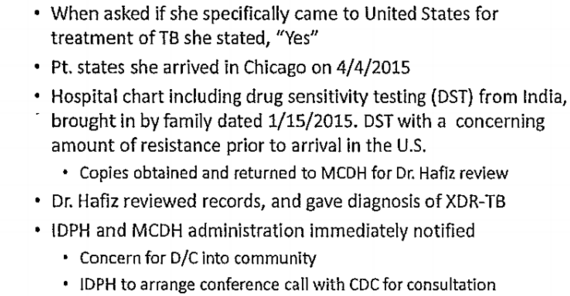
Woodstock Ill. — McHenry County Department of Health (MCDH) reports that on April 4 an individual from India infected with an extensively drug-resistant form of Tuberculosis, also known as XDR-TB, entered the United States and then traveled to other states.
On May 18, this individual visited family in McHenry County and, during this visit, sought treatment.
The patient has since been transferred out of state for care. Individuals who were in close contact with the patient have been interviewed and are being monitored.
Tuberculosis is not easily transmissible and XDR-TB, in particular, is also rare.
XDR-TB is a form of TB which is resistant to many of the most powerful anti-TB drugs.
According to the World Health Organization, developing XDR-TB is usually a sign of an active TB patient receiving inadequate clinical care or when a patient doesn’t receive the proper information, counseling and material support to complete their full course of treatment.
Tuberculosis is spread through the air by an infected person when coughing and sneezing.
People who are nearby may breathe in the TB bacteria and become infected.
TB is not spread by shaking someone’s hand, sharing food or drink, touching bed linens or toilet seats, sharing toothbrushes or kissing.
This is the first time MCDH has identified a case of XDR-TB in the County.
MCDH works closely with the Centers for Disease Control and Prevention, the Illinois Department of Public Health and local public health partners through its surveillance system to identify and monitor reportable infectious diseases in McHenry County.
In 2014, five active cases of TB (not XDR-TB) and 57 people with latent, non-infectious TB were treated.
MCDH’s Tuberculosis Clinic, located in Woodstock, provides chest x-rays, diagnostic studies, laboratory services and medication to any McHenry County resident in addition to outreach to those populations at high risk for developing TB.
If you think you have been exposed to someone with TB, contact your health care provider or MCDH to see if you should be tested. For more information on TB, call MCDH’s Communicable Disease Program at 815-334-4500
Posted in CDC, Centers for Disease Control, Contact Tracing, Illinois, McHenry County, McHenry County Health Department, Mike Hill, Susan Karras, TB Board, TB District, XDR-TB | 9 Replies
Above items are from: http://mchenrycountyblog.com/2015/11/25/mchenry-county-center-of-dangerous-tb-case/


By DENISE GRADYJUNE 9, 2015
Inside
Photo

Susan Karras, the communicable disease coordinator for McHenry County, outside Chicago, where a TB patient visited. Credit Steve Kagan for The New York Times
In the latest incident, a woman with TB flew from India to O’Hare International Airport in Chicago, landing on April 4. She traveled by car to visit relatives in Illinois, Tennessee and Missouri before seeking medical care sometime after May 18 at a hospital in Illinois. Tests there detected extensively drug-resistant tuberculosis, or XDR-TB. Doctors notified the state health department and the Centers for Disease Control and Prevention. The arduous task of contact tracing began in the three states.
Health officials say the risk to the public is low. TB is nowhere near as contagious as the flu or measles. But people who had long periods of close contact with the patient, like the relatives with whom she stayed, are at risk.
For people who were on the flight with the woman from India, the odds of catching TB are low but not zero. Cases have occurred in passengers on a long flight who sat near someone in advanced stages of the disease. In this case, the C.D.C. said, it will obtain the flight manifest for the woman’s trip from India and notify passengers who may have been exposed. An agency spokesman declined to reveal the airline or flight number.
Visitors from other countries are not screened for TB when they arrive, but those applying for legal residency are required to have TB tests, according to the C.D.C. Even if the government wanted to screen arriving passengers, it would be difficult, because there is no rapid test for tuberculosis.
On Friday, the patient from India was transferred to the National Institutes of Health in Bethesda, Md. In the past two decades, the N.I.H. has treated about 20 patients with drug-resistant TB, the most recent a year or so ago, according to Dr. Anthony S. Fauci, the head of the National Institute of Allergy and Infectious Diseases. Most came from other countries.
“Our track record has been good,” Dr. Fauci said, adding that about 80 percent were cured. That success rate is higher than the figures usually cited — 30 percent to 50 percent cured — because the lower estimates include results from poorer countries that have less access to drugs and other resources.
“This person is looking at a very long course of careful treatment and observation,” Dr. Fauci said.
Globally, nine million people contracted TB in 2013, and one and a half million died from it, according to the World Health Organization. Nearly a quarter of all the cases occurred in India, which has the world’s largest epidemic.
Over all, drug-resistant bacteria cause only about 5 percent of all cases, and XDR bacteria are a small subset of that group, causing about 48,000 cases in 2013. But XDR-TB has shown up in 100 countries, and it can be deadly, particularly in countries with weak health care systems.
So far, 12 people who had contact with the woman in Illinois have been identified, according to Susan Karras, the communicable disease coordinator for McHenry County, northwest of Chicago, the part of Illinois the patient visited. They were traced in 15 to 20 hours of interviews with the patient and her family at the hospital and by phone.
Some have had TB tests, but Ms. Karras declined to reveal whether any were positive. People whose initial results were negative will be tested again in about eight to 10 weeks, because the infection does not always show up on early tests.
Spokesmen for the Tennessee and Missouri health departments said contacts were being traced in those states, but did not provide any details.
Anyone who is infected will be treated, Ms. Karras said. In many people, TB can be latent, meaning that their immune systems keep the infection in check so they are not sick or contagious. But latent disease can become active. So even people with the latent form of the disease will be treated with whatever mix of potent drugs it takes to kill this particular strain of XDR-TB, she said.
“We want to treat it before it becomes infectious,” Ms. Karras said. “That’s why we want to find them.”
The woman from India is in isolation in a hospital at the N.I.H., Dr. Fauci said. She has no contact with other patients, and doctors and nurses who treat her must wear gloves, gowns, eye protection and specially fitted masks called N-95 respirators. Even though they take every precaution, health workers who treat TB patients are usually tested for the disease once a year, Dr. Fauci said.
At the N.I.H., patients with this kind of TB are usually kept in the hospital for weeks or even months, until sputum tests no longer find the bacteria, indicating that the disease is not contagious anymore, Dr. Fauci said.
Standard TB usually requires treatment with four drugs, which can take six to nine months. Treating XDR-TB takes longer, sometimes a year or more, and requires more drugs.
The drugs have unpleasant side effects that are hard to tolerate, Dr. Fauci said. They cause nausea, weakness and other problems that make patients want to quit taking them before the full course is finished. But missing doses and quitting too soon are precisely what cause drug-resistant bacteria to develop — requiring even longer treatment with more drugs and nastier side effects.
Sometimes in severe cases, surgery is needed to remove diseased and scarred parts of the lung harboring bacteria that the drugs cannot reach.
The patient will not be charged for her treatment. Even if patients are citizens of other countries, Dr. Fauci said, their governments are not billed.
“Everything is free at the N.I.H.,” he said. “No one pays.”
Dr. Fauci said that the woman’s treatment would be expensive, given the long stay and costly drugs needed, but that he could not even begin to estimate the ultimate cost.
Above is a from: http://www.nytimes.com/2015/06/10/health/indian-woman-being-treated-in-us-for-drug-resistant-tuberculosis.html?_r=2